 ქართული
ქართული
 English
English
 Русский
Русский
Blog
Esophageal hernia | Symptoms and surgery
Esophageal hernia | Symptoms and surgery

Esophageal hernia - what is this diagnosis and when is esophageal hernia surgery necessary?
Hiatal hernia is one of the most common, yet often poorly diagnosed, pathologies that affect the digestive system and quality of life. According to international epidemiological data, approximately 60% of people over the age of 50 have a small or medium-sized hiatal hernia - although many of them do not realize the true severity of the diagnosis for years. In this article, we will discuss in detail what an hiatal hernia is, what complications it causes without treatment, when esophageal hernia surgery is necessary, and how modern laparoscopic treatment is performed at the Bochorishvili Clinic. 
What is an esophageal hernia?
A hiatal hernia (or hiatal hernia) is a condition in which the upper part of the stomach or the esophageal-gastric junction protrudes into the chest cavity through a hole in the diaphragm called the hiatus. Normally, the diaphragm tightly separates the abdominal and thoracic cavities, and the esophagus protrudes through a narrow opening. When this opening weakens or widens, stomach contents migrate upward and the antireflux barrier is breached.
According to the international classification (Hill grading) , four types are distinguished:
- Type I - creeping, the most common (95% of cases);
- Type II - paraesophageal (the stomach fundus shifts to the side);
- Type III - combined;
- Type IV - complex, in which other organs are involved (small and large intestine
Correct identification of the type determines the treatment strategy and the urgency of surgery. 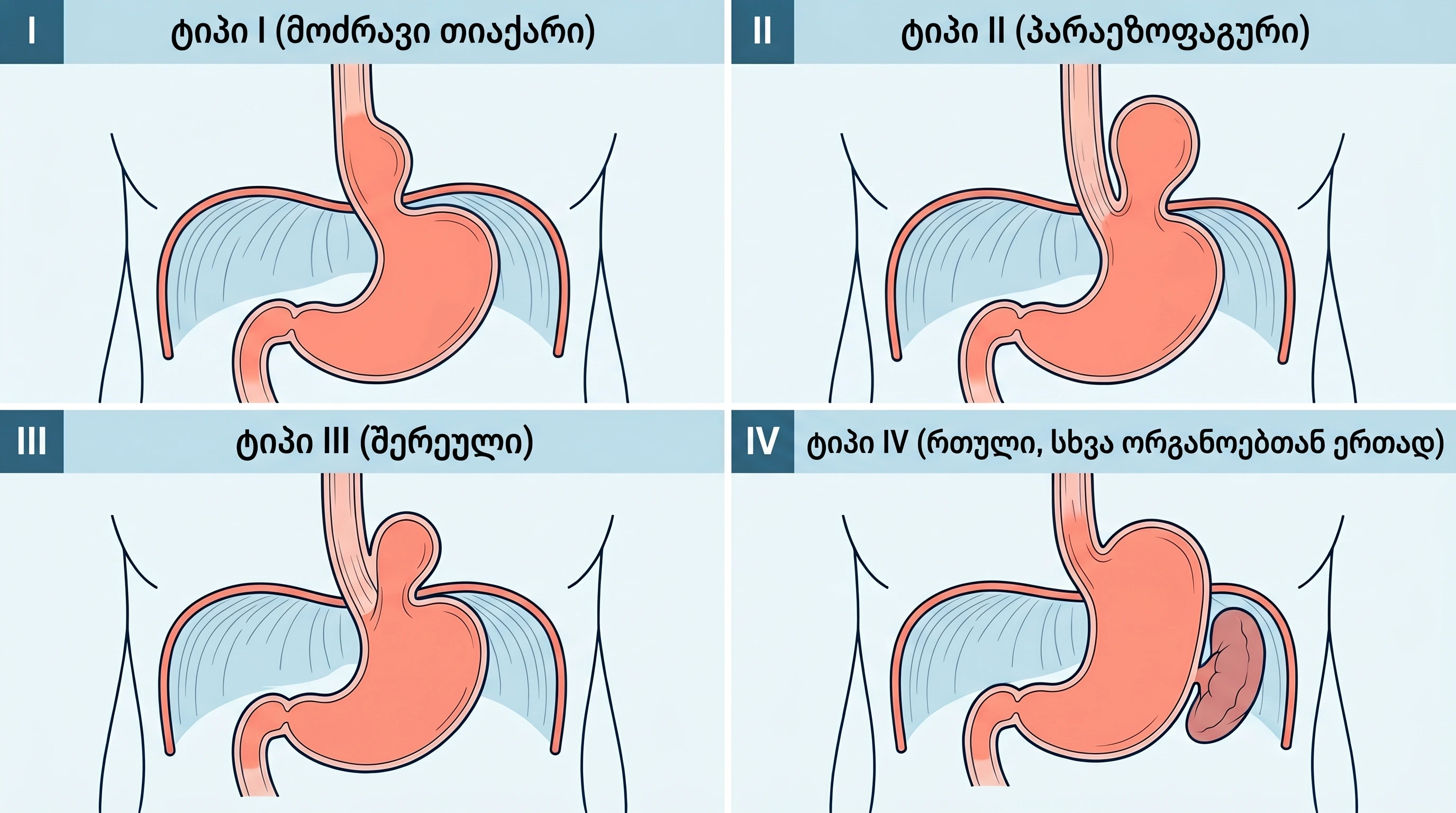
What causes an esophageal hernia?
A hiatal hernia is often caused by a combination of factors - factors that increase intra-abdominal pressure or weaken the diaphragm muscles.
The main risk factors are:
- Age over 50 years - natural aging of diaphragm tissues and changes in collagen structure;
- Overweight and obesity - persistent intra-abdominal pressure;
- Long-term cough (chronic bronchitis, asthma, smoking);
- Pregnancy - mechanical pressure from the enlarged uterus;
- Heavy physical exertion, especially incorrect lifting of weights;
- Chronic constipation and difficulty defecating;
- Genetic predisposition - anatomical features of the diaphragm;
- Smoking, which weakens the lower esophageal sphincter (LES).
In many cases, several factors act simultaneously, accelerating the development of hernias and early symptoms. The risk can often be reduced by controlling weight, adjusting the diet, and quitting smoking. 
What are the symptoms of an esophageal hernia?
A small hiatal hernia may be asymptomatic. Symptoms appear when the antireflux barrier is compromised or the hernia grows. The main signs are:
- Heartburn - often after eating, when lying down, or when the abdominal cavity is loaded;
- Pain behind the breastbone, which is sometimes mistaken for heart pain (so-called atypical chest pain);
- Return of a sour taste in the mouth (regurgitation);
- Difficulty swallowing (dysphagia), especially with solid foods;
- Frequent belching, feeling of bloating in the upper abdomen;
- Nighttime cough, hoarseness in the morning, chronic pharyngitis;
- Black stools (in severe cases, a sign of bleeding);
- Iron deficiency anemia of unknown origin.
If these symptoms recur regularly, a visit to the doctor is necessary. Large hernias, especially types II-IV, may not cause typical heartburn, but can provoke complications - so the absence of symptoms alone does not mean a safe condition. 
How is an esophageal hernia diagnosed?
The gold standard for diagnosis is a combination of a thorough clinical evaluation with specific instrumental studies:
- Esophagogastroduodenoscopy (EGD) - visual examination of the inside of the esophagus and stomach, evaluation of the mucosa, and the possibility of biopsy if necessary.
- Barium radiography - X-ray contrast study shows anatomical changes, size and type of hernia in dynamics.
- Esophageal manometry - an objective assessment of the pressure and motility of the lower esophageal sphincter.
- 24-hour pH monitoring - measuring the frequency and duration of reflux episodes.
- Chest CT with contrast - for a complete anatomical picture of type II-IV hernias, before planning surgery.
At Bochorishvili Clinic, these studies are performed with the latest equipment, using a unified multidisciplinary approach - which significantly reduces the time from diagnosis to treatment. 
What complications does an esophageal hernia cause without treatment?
An esophageal hernia left untreated will progress over time and lead to serious complications that are much more difficult to treat than elective surgery:
- Gastroesophageal reflux disease (GERD) - chronic acid reflux;
- Erosive esophagitis - inflammation of the esophageal mucosa, erosions and ulcers;
- Barrett's esophagus - a precancerous condition that increases the risk of esophageal adenocarcinoma by 30-40 times;
- Esophageal stenosis - a narrowing of the mucosa that makes it difficult to swallow;
- Iron deficiency anemia - a result of chronic minor bleeding;
- Entrapment - a medical emergency that requires immediate surgery;
- Aspiration and recurrent pneumonia - especially in the elderly.
These complications often require more complex and urgent surgical intervention, often an open surgery. 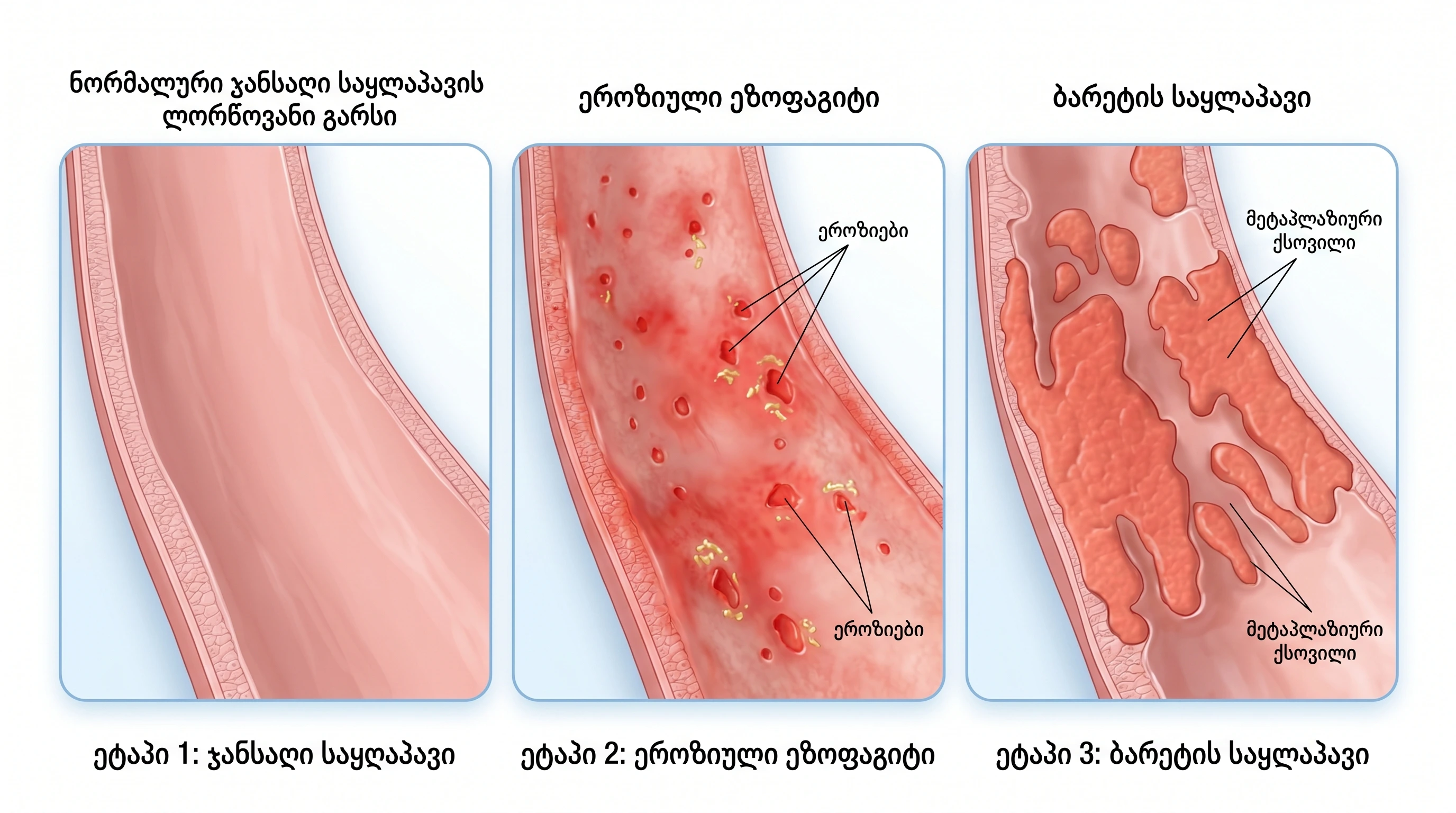
When is esophageal hernia surgery necessary?
Hiatal hernia surgery is recommended on an individual basis after a detailed assessment. According to international guidelines (SAGES, EAES), surgery is recommended when:
- 6-8 weeks of drug therapy (PPI or H2-blockers) does not provide symptom control;
- The patient cannot tolerate continuous medication treatment due to side effects;
- Erosive esophagitis, Barrett's esophagus, or esophageal stenosis is detected
- Diagnosed with a type II, III, or IV paraesophageal hernia - surgery is often recommended regardless of symptoms due to the high risk of complications;
- Recurrent aspiration or pneumonia;
- Severe symptomatic form at a young age - considering long-term quality of life.
The decision in favor of surgery is always based on the collegial recommendation of a multidisciplinary team (gastroenterologist, surgeon, anesthesiologist), which takes into account both medical and patient lifestyle factors.
How is esophageal hernia surgery performed?
Modern hiatal hernia surgery is most often performed laparoscopically - a minimally invasive method. This means 4-5 small (5-10 mm) incisions instead of open surgery , which means less bleeding, less pain, and smaller scars.
The operation (hiatal hernia repair + fundoplication) is performed in several stages:
- Returning the displaced portion of the stomach into its anatomical position within the abdominal cavity.
- Widened hiatus repair (crural repair) - suturing the diaphragm muscles and narrowing the hole.
- Fundoplication (Nissen 360° or Toupet 270°) - wrapping the fundus of the stomach over the lower part of the esophagus to restore the natural anti-reflux barrier.
- If necessary, use of synthetic or biological mesh for large defects to prevent recurrence.
The operation lasts 90-120 minutes , under general anesthesia. The patient is usually discharged from the hospital on the 2nd-3rd day . The mortality risk for laparoscopic fundoplication in specialized clinics is less than 0.2% . 
What to expect after esophageal hernia surgery?
The postoperative period after laparoscopic intervention is significantly different from open surgery:
- First 24-48 hours - follow a liquid regimen and slowly transition to soft foods;
- 1-2 weeks - semi-liquid or pureed food (strained soup, mashed potatoes, yogurt);
- 3-4 weeks - gradual transition to a normal diet, follow-up visit;
- 4-6 weeks - return to physical activity, gradual reduction in weight lifting.
Long-term result: Clinical studies have shown that laparoscopic Nissen fundoplication provides complete symptom control in 85-90% of patients even after 10 years. The need for ongoing PPI use is significantly reduced or eliminated. 
Why Bochorishvili Clinic for esophageal hernia surgery?
At Bochorishvili Clinic, esophageal hernia surgery is performed by a team of experienced laparoscopic surgeons, who combine many years of expertise and modern technologies:
- The latest HD+ 3D laparoscopic equipment and anesthesia techniques;
- Multidisciplinary approach - gastroenterologist, surgeon, anesthesiologist as a unified team;
- Individual treatment plan for each patient;
- Emergency 24-hour care in the postoperative period;
- Full diagnostic cycle in one space - from endoscopy to CT;
- European protocols (ERAS- Enhanced Recovery After Surgery) to reduce recovery time.
|
Consult at Bochorishvili Clinic If you or a loved one is suffering from heartburn, chest pain, or other symptoms of a hiatal hernia - don't delay. Book a consultation with our experienced laparoscopic surgery team. Website: bochorishvili.ge Contact: bochorishvili.ge/ka/contact |

Frequently asked questions about hiatal hernia
How long does esophageal hernia surgery last?
Laparoscopic hiatal hernia surgery usually lasts 90-120 minutes - the entire process, including preparation and anesthesia, is 2.5-3 hours. Hospital stay - 2-3 days.
Is it possible to treat an esophageal hernia without surgery?
Type I (creeping) small hernias are often controlled with lifestyle changes and medication (PPIs). However, types II-IV and treatment-resistant cases require surgical intervention, as medication only treats the symptoms, not the anatomical problem.
What are the risks of hiatal hernia surgery?
Laparoscopic fundoplication is a highly safe procedure performed in a specialized clinic. Possible risks: temporary dysphagia (5-10%), gas-bloat syndrome, in rare cases - esophageal damage or recurrence. The mortality risk is less than 0.2%.
What foods should I eat after surgery?
For the first two weeks - liquids and semi-liquid food: mashed potatoes, strained soup, yogurt, fruit puree. In 3-4 weeks, switch to soft food, then - to a regular diet. Avoid carbonated drinks, spicy foods and alcohol for at least 6 weeks.
Is it possible for an esophageal hernia to recur after surgery?
The risk of recurrence after laparoscopic fundoplication is 5-10% over 10 years . The risk is reduced by proper surgical technique, the use of mesh for large defects, and patient compliance with recommendations (weight control, smoking cessation, avoidance of inappropriate loading).
Medical Warning: This article is for informational purposes only and is not a substitute for the advice of a qualified physician. Diagnosis and treatment plans are determined on an individual basis, after a complete evaluation of the patient.