 ქართული
ქართული
 English
English
 Русский
Русский
Blog
Bariatric surgery - modern treatment of obesity
Bariatric surgery - modern treatment of obesity

Table of contents
- What is bariatric surgery?
- Who needs bariatric surgery? - BMI criteria
- Types of bariatric surgery
- Advantages of laparoscopic surgery
- Preoperative preparation
- Rehabilitation and nutrition after surgery
- Risks and complications
- Why Bochorishvili Clinic?
- Frequently Asked Questions (FAQ)
- Scientific sources
What is bariatric surgery?
Bariatric surgery is a surgical treatment method for obesity that aims to achieve both weight loss and remission of obesity-related diseases.
According to the World Health Organization (WHO), more than 40% of adults struggle with obesity.
Obesity is associated with:
- Type II diabetes;
- Cardiovascular diseases;
- Arterial hypertension;
- Obstructive sleep apnea;
- dyslipidemia;
- Certain types of oncological diseases;
- Infertility.
Often, it is precisely these comorbidities that make bariatric surgery necessary.
Bariatric surgery is not a cosmetic treatment, nor is it a substitute for a healthy lifestyle. It is a medical intervention that is performed according to strictly defined criteria and is based on essential needs.
Who needs bariatric surgery? - BMI criteria
According to the guidelines of the International Federation of Bariatric and Metabolic Surgery (IFSO) and the American Society of Metabolic and Bariatric Surgery (ASMBS), bariatric surgery is recommended in the following cases:
- BMI ≥ 40 kg/m² - morbid obesity regardless of comorbidities;
- BMI 35-39.9 kg/m² - obesity with one or more comorbidities (type II diabetes mellitus, arterial hypertension, dyslipidemia, obstructive sleep apnea, obesity-related hypoventilation syndrome, severe osteoarthritis);
- BMI 30-34.9 kg/m² - Untreated type II diabetes or metabolic syndrome;
- Unsuccessful course of conservative treatment for at least 6 months - proper nutrition, physical activity, drug therapy.
However, checking the BMI criterion is only the first step. The bariatric protocol at Bochorishvili Clinic takes into account two other important psychological factors:
- Realistic understanding of the risks and outcomes of the surgery - the patient must understand that the process following bariatric surgery largely depends on him/herself. Bariatric surgery makes it easier to maintain a calorie balance, however, in order to achieve the final result, the patient must maintain discipline and follow the recommendations meticulously.
- Readiness for a radical lifestyle change - According to medical literature, 15-25% of patients regain the weight they lost within 5 years if they do not follow the recommended nutritional and physical activity standards.
Bariatric surgery doesn't mean eliminating diet and exercise — it means making them more effective at getting the most out of small portions.
Types of bariatric surgery
The multidisciplinary team of Bochorishvili Clinic selects the type of surgery individually, taking into account the patient's BMI, concomitant diseases, anatomical features, and lifestyle.
Sleeve gastrectomy
Sleeve gastrectomy - is the most common bariatric surgery method in the world today. During this procedure, 70-80% of the stomach is removed, leaving a tubular structure with a diameter of 1-1.5 cm.
The result works through two mechanisms:
- Mechanical - the stomach volume is reduced from approximately 1500-2000 ml to 150-200 ml, which limits the amount of food intake;
- Hormonal - the hunger hormone ghrelin accumulates in the removed part of the stomach. By removing this part, appetite is significantly reduced not at the expense of the patient's willpower, but at a physiological level.
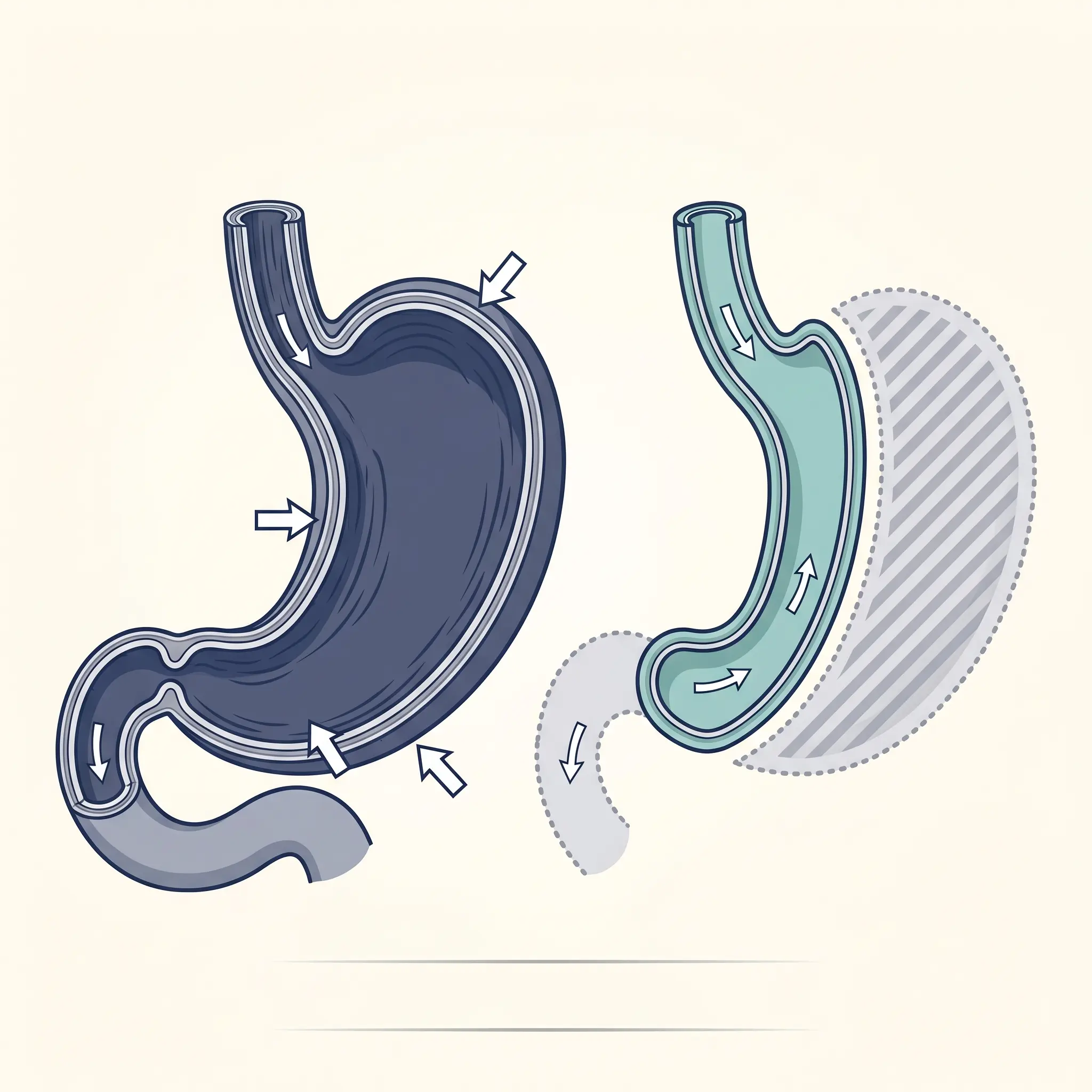
Sleeve gastrectomy is preferred for patients with a BMI ≥ 40 kg/m² and for those for whom alteration of intestinal anatomy is conceptually unacceptable.
Gastroscopy
Gastric bypass surgery — also known as "classic bypass" or Roux-en-Y — is considered the gold standard by many bariatric surgeons, especially in cases of high BMI ≥ 50 kg/m² and comorbid diabetes.
The operation includes two components:
- Restriction - the upper part of the stomach becomes smaller and separates from the rest of the stomach. A 30-40 ml reservoir is created - which significantly limits the amount of food intake;
- Malabsorption - A portion of the small intestine is cut off and connected to the stomach in a way that prevents the absorption and full utilization of nutrients.
This combination provides a significant metabolic effect - according to scientific studies, in 80-85% of cases, type II diabetes goes into remission soon after gastric bypass surgery. Often even within a few days of surgery. Gastric bypass is a complex procedure, but both the weight loss process and the results are more sustainable, often within a few days of surgery.
Mini gastric bypass (mini bypass)
Mini Gastric Bypass is a simplified version of the classic bypass. It is a single-anastomosis (one connection point) operation, which reduces operating time, the risk of anastomotic complications, and makes the operation reversible.
Mini-bypass is particularly effective for patients with a BMI of 40-55 kg/m² who have type 2 diabetes or severe dyslipidemia.
Gastric banding
Gastric banding is the first widely used method of bariatric surgery. In this procedure, a special silicone ring is fixed to the upper part of the stomach, which divides the stomach into two parts. A narrow passage is created between these parts, which allows for a small portion of food to be eaten.
Nowadays, gastric banding surgery is performed less and less often, as the results are unstable (weight maintenance occurs in only 40-50% of cases). It is noteworthy that over time, the band may shift in position as it moves.
Biliopancreatic shunt (BPD/DS)
Biliopancreatic bypass surgery is known as the most complex and most effective bariatric surgery for super-morbid obesity (BMI 50+). kg/m²). It involves significant reduction of the stomach and radical bypass of the small intestine.
Result: 70-80% of the weight lost is maintained for 10-15 years. However, the surgery requires continuous monitoring to prevent vitamin and mineral deficiencies - especially fat-soluble vitamins (A, D, E, K), iron, calcium, and B12.
Endoscopic methods - gastric ballooning and Botox
In addition to surgical interventions, endoscopic bariatric methods are available at Bochorishvili Clinic:
- Gastric ballooning - a balloon capsule is inserted into the stomach through the mouth, the patient swallows the capsule, and then it is filled with saline solution to 400-600 ml. The balloon occupies a large part of the stomach, which causes a decrease in appetite and a constant feeling of fullness. After 6 months, the balloon is removed from the stomach. This method is optimal for patients with a BMI of 27-35 kg/m², or for weight loss before bariatric surgery.
- Stomach Botox - Endoscopic Stomach Botox is one of the simplest and most modern methods. During which botulinum toxin is injected endoscopically into the stomach wall - the volume of the stomach decreases, slowing down motility and prolonging the feeling of fullness. The effect lasts for 4-6 months. Stomach Botox is considered for patients with a BMI of 27-32 kg/m².
Advantages of laparoscopic surgery
In the modern world, bariatric surgery has almost completely shifted to the laparoscopic method. Nowadays, open bariatric surgery is considered only in cases of absolute necessity.
Advantages of laparoscopic bariatric surgery:
- Minimal trauma - 5-6 small (5-12 mm) incisions instead of the 15-20 cm incision of open surgery;
- Fast recovery - the patient stays in the clinic for 1-2 days, usually able to move independently within 6-12 hours ;
- Low risk of infection due to small wounds;
- Minimal scarring - an aesthetic advantage, especially for young patients;
- Low risk of hernia development - the risk of a hernia occurring is less than 1%, while in the case of open surgery the risk probability reaches 10–15%;
- Better viewing conditions for the surgeon - especially when using a 3D laparoscope.
The operating room of the Bochorishvili Clinic is equipped with the world's most advanced 3D video laparoscope , which provides the surgeon with three-dimensional, natural color visual information. This technology reduces the risk of intraoperative errors, facilitates the rapid course of the procedure, and is especially useful in patients with complex anatomy - when fatty tissue limits the clear visibility of anatomical structures.
Preoperative preparation
The bariatric protocol does not start on the operating table. At Bochorishvili Clinic, the decision is made by a multidisciplinary team, which includes:
- Bariatric surgeon - selection of surgery strategy;
- Endocrinologist - assessment of hormonal profile, stabilization of concomitant metabolic diseases;
- Nutritionist - lifestyle assessment and eating habits change plan ;
- Psychotherapist - psychological readiness assessment and screening for eating disorders;
- Gastroenterologist - evaluation of the gastric mucosa through endoscopic examination;
- Cardiologist and anesthesiologist - assessment of the risks of surgical complications.
Preoperative studies include:
- Blood and urine tests;
- Biochemical studies;
- Hormonal profile (TSH, insulin, cortisol);
- Determination of vitamin D and B12 levels;
- Electrocardiography (ECG);
- Echocardiography;
- Pulmonary function testing;
- Ultrasound examination of the liver and biliary tract;
- Gastroscopy (stomach endoscopy) with Helicobacter pylori screening.
2-4 weeks before surgery, the patient is prescribed a special diet - a high-protein, low-fat diet that reduces the size of the liver and facilitates laparoscopic visualization during surgery.
Rehabilitation and nutrition after surgery
Rehabilitation after bariatric surgery lasts 4-6 weeks, and major weight loss is achieved within 12-18 months.
Postoperative phases
|
Phase |
Time | Food |
|---|---|---|
| Phase 1 | 1-7 days | Liquids: water, broth, juice (without sugar) |
| Phase 2 | 8-21 days | Puree - blended food |
| Phase 3 | 22-30 days | Soft and crumbly food |
| Phase 4 | 30+ days | Regular food in small portions |
Basic nutrition guidelines after bariatric surgery
- Small portions 4-6 times a day - due to reduced stomach volume;
- Protein-rich foods - it is advisable to consume at least 60-80 grams of protein per day (meat, fish, eggs, dairy products, protein supplements);
- Separate fluids and food - A common mistake is to drink fluids with meals, which speeds up stomach emptying. It is recommended to drink fluids 30 minutes before meals or 30 minutes after meals;
- Vitamin-mineral supplements for the rest of life - B12, vitamin D, iron, calcium, zinc;
- Alcohol prohibition - especially during the first year. Alcohol absorption in bariatric patients occurs much faster and more intensively, which increases the risk of addiction;
- Physical activity - walking is recommended 30 days after surgery, moderate exercise from 6 weeks;
- Psychological support - especially during the first 6 months, when the body and social self-perception are changing.
Risks and complications
Any surgical intervention is associated with certain risks. It is necessary to correctly assess the risks and provide the patient with meticulously accurate information. The doctors of the Bochorishvili Clinic minimize all possible risks as much as possible.
Early complications (first 30 days):
- Anastomotic rupture/leakage - 1-2% of cases;
- Bleeding - 1-3%;
- Deep vein thrombosis/pulmonary embolism - 0.5-1%;
- Wound infection - 1-2%;
- Anesthetic complications - < 1%.
Late complications:
- Vitamin and mineral deficiencies - occur in 30-50% of cases within the first 5 years if the patient does not take supplements;
- Dumping syndrome - especially after gastric bypass surgery, when consuming sugar;
- Gallstones - in 25-30% of cases as a result of rapid weight loss;
- Weight regain - 15-25% of cases within 5-10 years;
- Psychoemotional changes - depression, difficulty adapting to lifestyle changes.
The risk of mortality in modern bariatric surgery is 0.1-0.3% - it is worth noting that this is lower than the risk of gallbladder removal (0.5%) or knee replacement surgery (0.4%).
Why Bochorishvili Clinic?
Bariatric surgery is not a decision that a patient should make based solely on price comparison. The final decision should be based on the experience of the clinic, the professionalism of the team, and the results of the treatment.
Three main advantages of Bochorishvili Clinic:
- Legacy of medical traditions - The clinic was founded in 1979 as an anti-sepsis center. Through the efforts of professional doctors, sepsis mortality in Georgia has decreased from 65% to 5% - a medical culture that is based on evidence-based clinical protocols and does not change over time.
- A professional multidisciplinary team - a team of doctors operates according to a bariatric protocol, which includes:
- Bariatric surgeon;
- Endocrinologist;
- Psychotherapist;
- Gastroenterologist;
- Cardiologist;
- Anesthesiologist.
- Technological equipment - The clinic's operating room is equipped with the world's most advanced 3D laparoscope - a technology that provides the surgeon with three-dimensional visualization and significantly reduces the risk of intraoperative error.
For any information about bariatric surgery, call us and schedule an initial consultation.
- Phone: 032 2 312 112; 577 222 112
- Address: Tbilisi, Al. Kazbegi Avenue 16
- Website: bochorishvili.ge
Frequently Asked Questions (FAQ)
How much does bariatric surgery cost in Georgia?
The cost of bariatric surgery depends on the type of surgery and includes preoperative studies, surgery, hospitalization, and postoperative monitoring. Sleeve gastrectomy is usually more affordable than gastric bypass. The exact cost is determined after the initial consultation, depending on the surgical approach chosen.
How much weight will I lose after bariatric surgery?
On average, a bariatric patient loses 60-80% of their excess weight in the first 18 months. This means that if a patient weighs 130 kg instead of the ideal 75 kg (overweight 55 kg), they will lose 33-44 kg.
Is bariatric surgery safe?
The risk of mortality in modern bariatric surgery centers is 0.1-0.3%, which is lower than in standard surgical operations. However, any operation involves risk. The decision should be made only after evaluation by a multidisciplinary team.
Is bariatric surgery possible in minor patients?
Bariatric surgery is rarely considered under the age of 18, only in cases of extreme morbid obesity and severe comorbidities, in strict compliance with international pediatric guidelines.
Will I regain the weight I lost in the future?
It is possible to regain the weight you lost if you do not change your lifestyle. According to scientific studies, 15-25% of bariatric patients experience weight regain within 5-10 years, mainly due to reasons related to eating habits.
Will I have a scar on my stomach?
Laparoscopic bariatric surgery is performed through 5-6 small (5-12 mm) incisions, the traces of which become practically invisible after 6-12 months.
How safe is pregnancy after bariatric surgery?
Yes, although it is recommended to postpone pregnancy for at least 12-18 months after surgery - until weight has stabilized and nutritional status has been restored. Bariatric surgery often resolves infertility problems as well.
Which is better - a sleeve or a bypass?
There is no clear and precise answer to this. Sleeve gastrectomy is technically a relatively simple operation and does not require intestinal bypass. It is recommended for patients with a BMI of 40-50 kg/m². Gastro bypass is a relatively complex operation, but more effective in cases of super-morbid obesity and concomitant diabetes mellitus. The final decision is made by the bariatric team individually, depending on the need.
Scientific sources
- World Health Organization. Obesity and overweight. WHO Fact Sheet, 2024.
- International Federation for the Surgery of Obesity and Metabolic Disorders (IFSO). Indications for Bariatric Surgery. 2022 Position Statement.
- American Society for Metabolic and Bariatric Surgery (ASMBS). Estimate of Bariatric Surgery Numbers, 2011-2023. ASMBS Public Health Statement.
- Mingrone G, et al. Metabolic Surgery versus Conventional Medical Therapy in Patients with Type 2 Diabetes: 10-Year Follow-Up of an Open-Label, Single-Centre, Randomized Controlled Trial. The Lancet, 2021.
- Schauer PR, et al. Bariatric Surgery versus Intensive Medical Therapy for Diabetes - 5-Year Outcomes (STAMPEDE Trial). New England Journal of Medicine, 2017.
- Eisenberg D, et al. 2022 ASMBS/IFSO Guidelines on Indications for Metabolic and Bariatric Surgery. Surgery for Obesity and Related Diseases, 2022.
This article is for general informational purposes only and is not a substitute for individual medical advice. Before making a decision about bariatric surgery, please schedule a personal consultation with the bariatric team at Bochorishvili Clinic.