 ქართული
ქართული
 English
English
 Русский
Русский
Blog
Allergy - symptoms, causes, diagnosis and treatment
Allergy - symptoms, causes, diagnosis and treatment

Modern Allergology: Approaches and Prevention
Allergy is one of the most common diseases in the modern world, affecting approximately 30-40% of the world's population ( World Allergy Organization, 2026 ). An allergy is an exaggerated response of the immune system to substances that are harmless to a healthy human body. This article covers:
- Scientific discussion of various forms of allergies;
- Modern diagnostic methods;
- Current treatment approaches;
- Practical recommendations for prevention.
What is an allergy?
It is a pathological hypersensitivity reaction of the immune system to normally harmless substances in the environment, called allergens. From an immunological point of view, an allergic reaction belongs to the type I (IgE-mediated) hypersensitivity reaction according to the classification of Gel and Coombs. 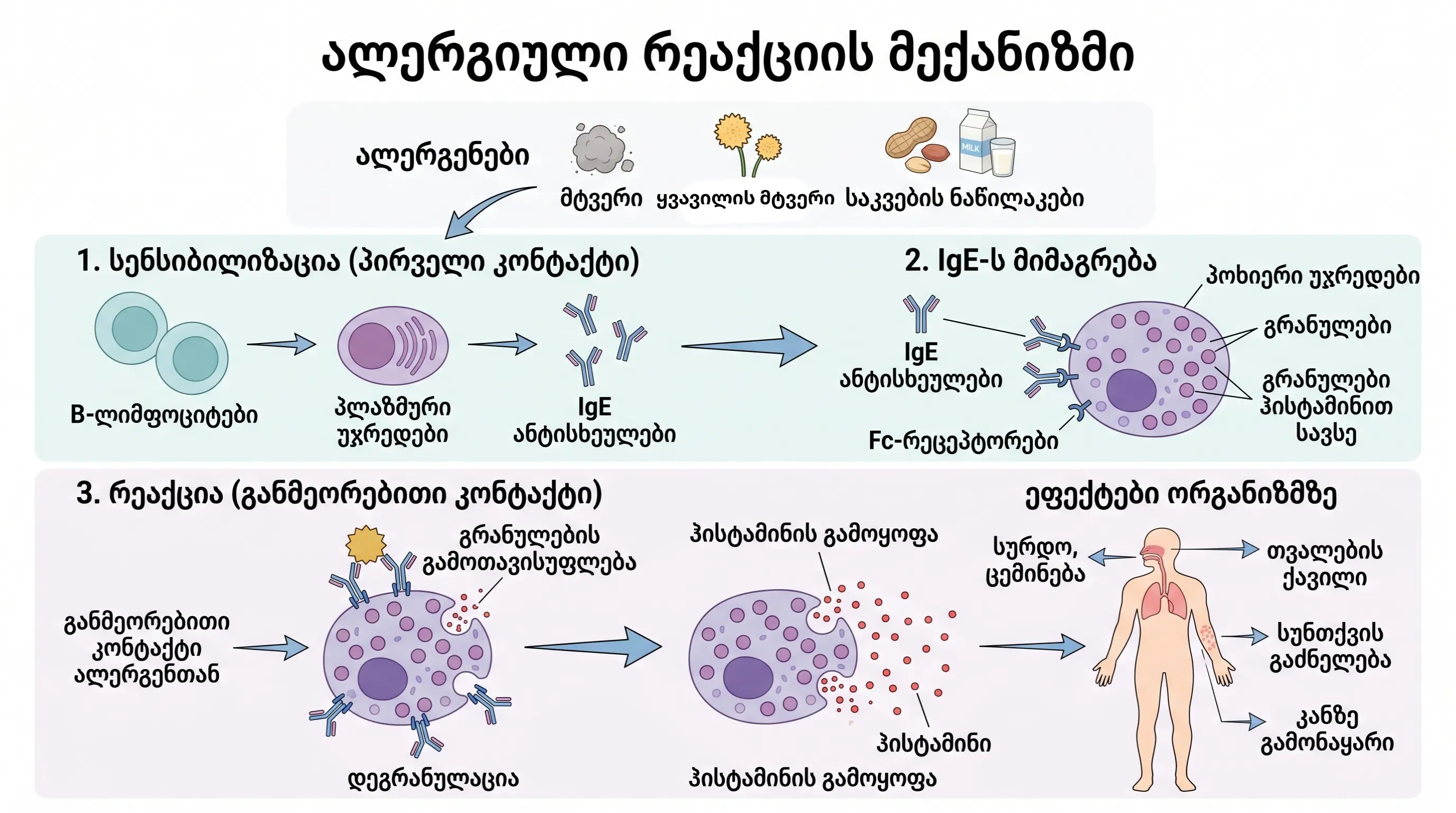
The mechanism of an allergic reaction in stages:
1 Sensitization - the body encounters an allergen for the first time and the immune system produces specific IgE antibodies.
2 Attachment - IgE antibodies attach to the surface of mast cells and basophils.
3 Recognition - Upon repeated contact with the allergen, IgE antibodies recognize the allergen.
4 Degranulation - Mast cells release inflammatory mediators:
- Histamine;
- Leukotrienes;
- Prostaglandins;
- Other bioactive substances.
5 Symptoms - Inflammatory mediators cause allergic clinical manifestations.
5 main categories of allergens:
- Respiratory - dust, pollen, mold spores, animal keratin;
- Food - milk, eggs, fish, soy, nuts, seafood, etc.;
- Contact - nickel, latex, cosmetics, etc.;
- Medication - antibiotics, nonsteroidal anti-inflammatory drugs;
- Insect venom - bee, hornet, wasp sting.
Genetic risk factors (atopy):
- If one parent has an allergy, the probability of the child developing it is 25-30% .
- In the case of both parents - the risk increases to 60-70% ( Thomsen, 2015, Clinical & Experimental Allergy ).
How to recognize an allergy
Identifying an allergy requires a systematic assessment of symptoms and their association with possible triggers. The clinical manifestations of an allergic reaction are diverse and depend on the type of allergen, the route of its entry into the body, and individual sensitivity.
.webp)
Symptoms by system:
1. Respiratory symptoms:
- Nasal congestion;
- Sneezing (especially serial);
- Watery discharge from the nose;
- Burning and tearing of the eyes;
- Itching and irritation of the throat.
2. Skin symptoms:
- Itching (intense or moderate);
- Red rash;
- Hives (urticaria);
- swelling;
- Eczema rash.
3. Gastrointestinal symptoms:
- Nausea;
- Vomiting;
- Abdominal pain/cramps;
- Diarrhea;
- Itching of the mouth (oral allergy syndrome).
4. Systemic symptoms (anaphylaxis):
- Drop in blood pressure;
- Difficulty breathing;
- Nausea and dizziness;
- Loss of consciousness.
5 signs that distinguish allergies from a viral cold
| Sign | Allergy | Cold |
| 1. Temperature | It does not increase. | Often increased |
| 2. Discharge | Transparent, like water | Yellow or green |
| 3. Duration | Weeks-months | 7-10 days |
| 4. Itching (eyes/nose) | Intensive | Rare |
| 5. Seasonality | Expressed | Doesn't have |
3 main keys to recognizing it:
- Seasonality - symptoms appear at the same time each year;
- Situational - symptoms are associated with a specific environment (dusty room, flowering season, certain foods);
- Reversibility - symptoms disappear when contact with the allergen is stopped.
How to understand what we are allergic to
Identification of the causative allergen is a critical step in clinical diagnosis. Modern allergology uses several validated methods. 
5 main methods of allergy diagnosis:
1. Skin Prick Test (SPT)
- Status: "Gold standard" of allergy diagnostics.
- Procedure: A drop of allergen extract is placed on the skin of the forearm and a superficial prick is made with a small needle.
- Result time: 15-20 minutes.
- Positive reaction: papule ≥3 mm + hyperemia.
- Sensitivity: 70-95%.
- Specificity: 85-95%.
2. Blood test (Specific IgE, ImmunoCAP)
- Measures the concentration of allergen-specific IgE antibodies in the blood.
- It is especially useful when skin testing is not possible.
- In the presence of severe dermatitis.
- While taking antihistamine medications.
- At high risk of anaphylaxis.
3. Provocation test
- Delivery of the allergen under controlled conditions.
- Routes of delivery: inhalation, oral or cutaneous.
- Used when results from other tests are inconclusive.
- It is carried out only under medical supervision.
4. Elimination diet (for food allergies)
- Removing the suspected allergen from the diet for 2-4 weeks.
- Monitoring symptoms during the elimination period.
- Gradual return of the allergen.
- Recording the recurrence of symptoms.
5. Patch Test
- Specifically for diagnosing allergic contact dermatitis.
- The allergen is attached to the skin of the back for 48 hours.
- The reaction is assessed after 48 and 96 hours.
- Tests 20-80+ contact allergens simultaneously.
Allergic cough
Allergic cough is a manifestation of airway hyperreactivity that develops as a result of inhalation contact with an allergen. 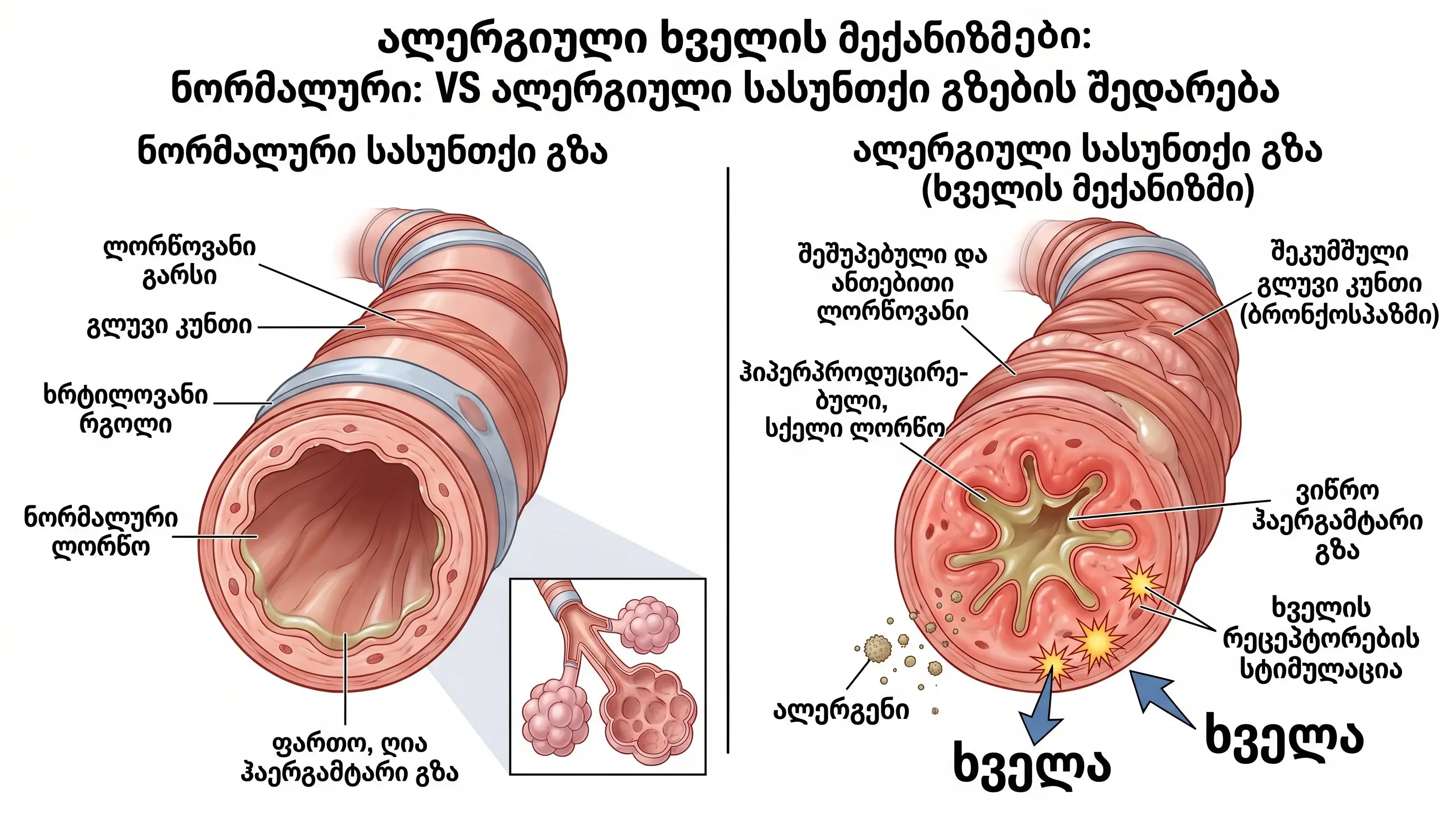
Pathophysiological mechanism:
- Inhalation of allergen;
- Activation of eosinophilic inflammation;
- Swelling of the bronchial mucosa;
- Mucus hypersecretion;
- Bronchospasm;
- Stimulation of the cough reflex.
6 distinctive signs of an allergic cough:
- Dry, unproductive character (a small amount of clear sputum is possible);
- Seasonal or situational exacerbation;
- Expressing at night or early in the morning;
- Duration more than 3 weeks;
- Resistance to antibiotics;
- Accompanying allergic symptoms (sneezing, nasal congestion).
| Reason | Characteristic sign |
| 1. Allergic cough | Seasonal, dry, responds to antihistamines |
| 2. Infectious cough | Temperature, purulent sputum, 1-3 weeks |
| 3. Reflux cough | Burning in the chest after eating |
| 4. Cough asthma | At night, during physical activity |
Treatment regimen:
- First line: Minimize allergen exposure;
- Second line: inhaled corticosteroids (budesonide, fluticasone);
- Third line: antihistamine drugs;
- Fourth line: leukotriene receptor antagonists (montelukast);
- Severe cases: bronchodilators.
Important: Allergic cough often precedes the development of allergic asthma - this concept is known as the "Allergic March".
Skin allergy
Skin allergy (allergodermatosis) encompasses a wide range of allergic skin reactions and is one of the most common forms of allergic diseases. According to EAACI , approximately 20% of the population will develop some form of skin allergy during their lifetime.

4 main clinical forms:
1 Atopic dermatitis (eczema)
- Chronic, relapsing inflammatory disease.
- It is characterized by intense itching, dry skin, and eczematous rashes.
- Has a genetic predisposition (atopic triad).
2 Allergic contact dermatitis
- It develops as a result of direct skin contact with an allergen.
- Common allergens are:
- Nickel (jewelry, belt buckle).
- Latex (gloves).
- Perfumes and preservatives.
- Chrome (leather goods).
3 Hives (urticaria)
- Raised, itchy blisters appear on the skin, which appear and disappear in a short period of time (minutes to hours).
- It is characterized by a migratory nature.
- It can be acute (<6 weeks) or chronic (>6 weeks).
4 Angioedema
- Deep subcutaneous edema.
- Localization: lips, eyelids, tongue, larynx.
- It may be life-threatening (due to airway obstruction).
- May be IgE-mediated or bradykinin-mediated.
3 central factors of pathogenesis:
- Skin barrier disruption - filaggrin gene (FLG) mutation (in 30-50% of atopic dermatitis cases);
- Immune dysregulation - Th2-biased immune response;
- Environmental factors - penetration of allergens through a broken barrier.
( Palmer et al., 2006, Nature Genetics )
Allergic rash
An allergic rash is an inflammatory skin reaction that develops in response to an allergen by the immune system. 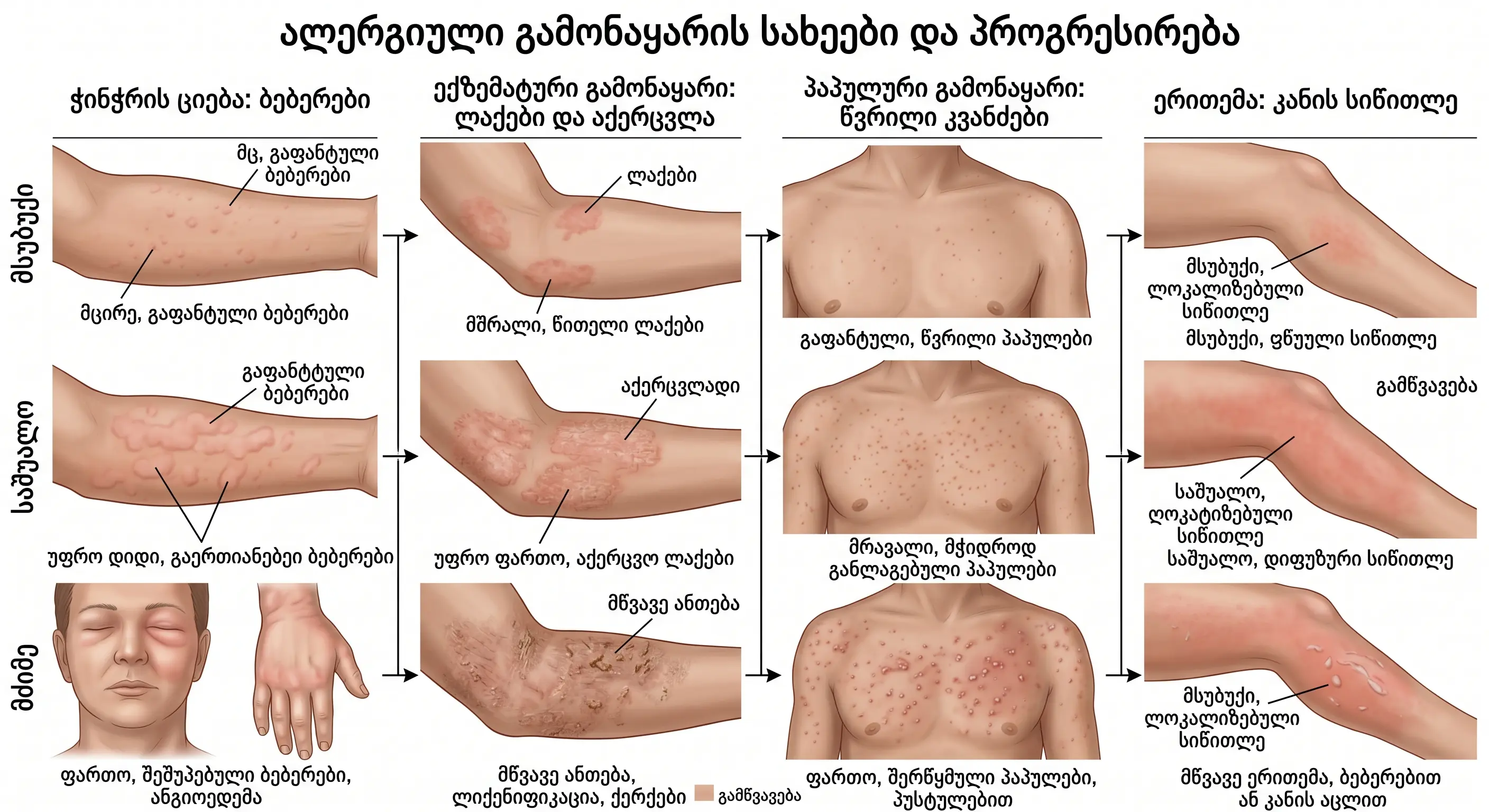
Morphological types of rashes:
- Erythema - redness of the skin (dilation of capillaries);
- Papules - raised, firm nodules (<1 cm);
- Vesicles - fluid-filled blisters (<1 cm);
- Urticaria blisters - elements of hives;
- Eczematous plaques - scaly, itchy elements.
4 characteristic signs:
- Intense itching - the main symptom;
- Symmetrical arrangement - the same on both sides;
- Regression - decreases when contact with the allergen is stopped;
- Relapse - occurs again upon re-exposure.
Differential diagnosis - what should we distinguish from:
- Infectious rash (viral exanthema, fungal infection);
- Autoimmune rashes (psoriasis, lupus);
- Other dermatoses (seborrheic dermatitis, rosacea).
4 stages of treatment:
1 Identification and elimination of the allergen - the basis of treatment.
2 Topical therapy:
- Corticosteroids (hydrocortisone, betamethasone);
- Moisturizing emollients to restore the skin barrier.
3 oral antihistamines (cetirizine, loratadine).
4 Refractory cases:
- Calcineurin inhibitors (tacrolimus, pimecrolimus);
- Systemic immunomodulators.
Allergy to dust
Dust allergy (household dust allergy) is the most common cause of allergic rhinitis. 
Basic facts about dust mites:
- Species: various types of dermatophytes;
- Allergen: not the mite itself, but its fecal particles;
- Proteins: Der p 1, Der f 1 - strong allergens;
- Optimal conditions: 20-25°C, 70-80% humidity;
- Concentration: 100-500 mites per gram of dust.
Where do dust mites gather?
- Mattresses and mattresses;
- Pillows;
- Soft furniture (sofa, armchair);
- Carpets;
- Curtains and heavy fabrics;
- Soft toys.
Symptoms of dust allergy:
- Chronic nasal congestion;
- Sneezing (especially in the morning, upon waking);
- Itching and tearing of the eyes;
- Itchy nose;
- Exacerbation of bronchial asthma (in sensitized patients);
- Deterioration in sleep quality.
7 effective ways to prevent:
- Using anti-allergenic covers on mattresses and pillows;
- Weekly washing of linen at a temperature of ≥60°C;
- Keeping humidity below 50%;
- Removing carpets - preference for hard floors;
- Using a vacuum cleaner with a HEPA filter ;
- Minimize or regularly wash soft toys ;
- Install an air purifier in the bedroom.
( Custovic et al., 2015, JACI - Combined measures significantly reduce allergen exposure )
Rash on the face
Allergic rashes on the face require special clinical attention because the skin on the face is thinner and more sensitive than the skin on other areas of the body. 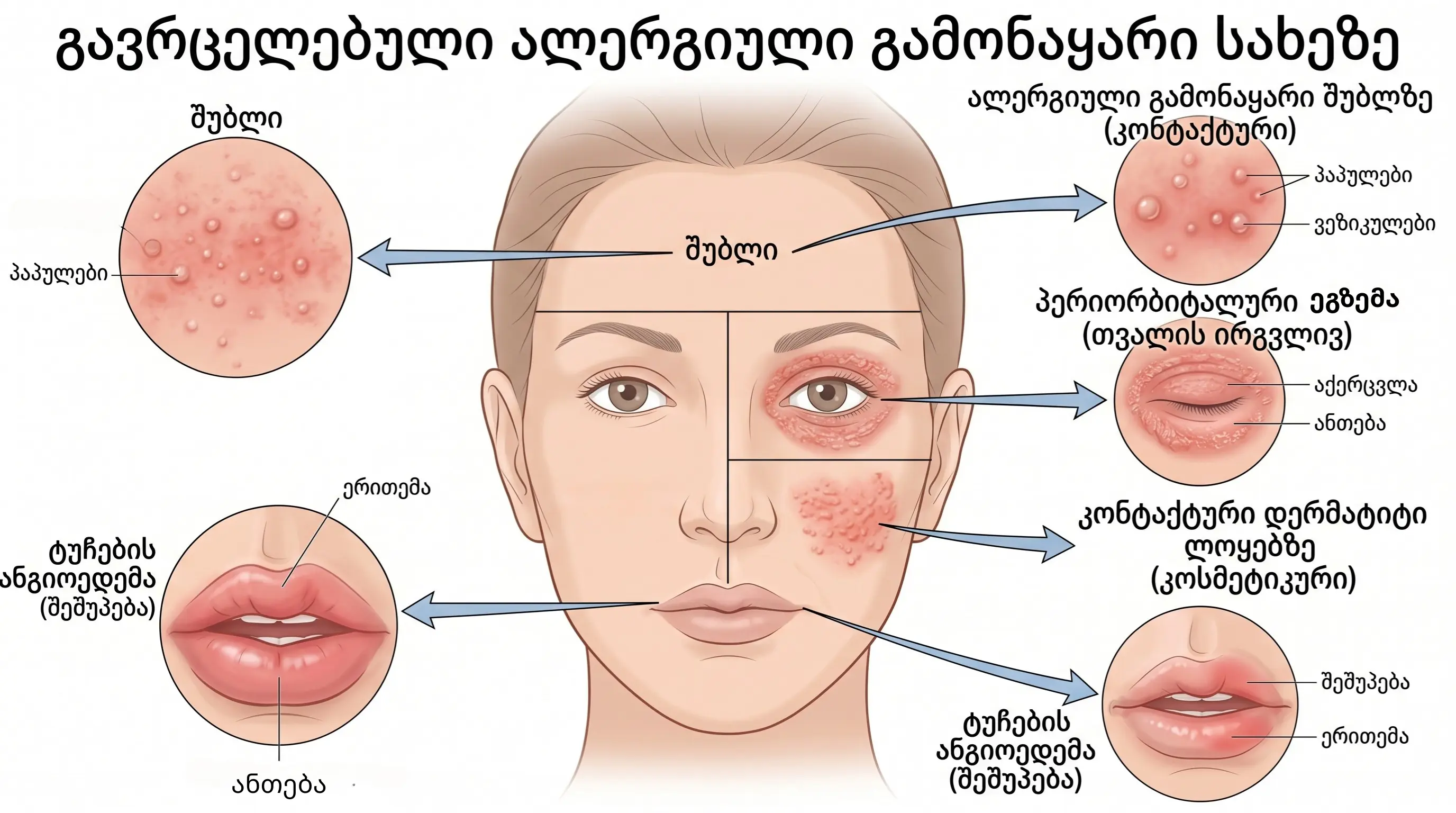
4 common triggers:
- Cosmetics and perfumes;
- Food allergens;
- Aeroallergens;
- Ultraviolet radiation.
Clinical forms:
- Periorbital eczema - redness, swelling, scaling around the eyes;
- Malar erythema - symmetrical redness on the cheeks;
- Angioedema - deep swelling of the lips, eyelids, or face;
- Contact dermatitis - a localized rash in the area of cosmetic application.
Treatment principles:
1 Recommended drugs:
- Non-fluorinated, weakly active topical corticosteroids (hydrocortisone 1%);
- Calcineurin inhibitors (tacrolimus 0.03%).
2 Why not strong steroids? Facial skin is particularly sensitive to side effects:
- Skin atrophy;
- Telangiectasia (appearance of blood vessels);
- Perioral dermatitis.
3 Preventive measures:
- Use of hypoallergenic cosmetics;
- Choosing fragrance-free products;
- Testing a new product on the wrist 24 hours in advance;
- Regular use of a protective cream containing SPF.
Allergic dermatitis
Allergic dermatitis (atopic dermatitis/eczema) is a chronic, relapsing, inflammatory skin disease. 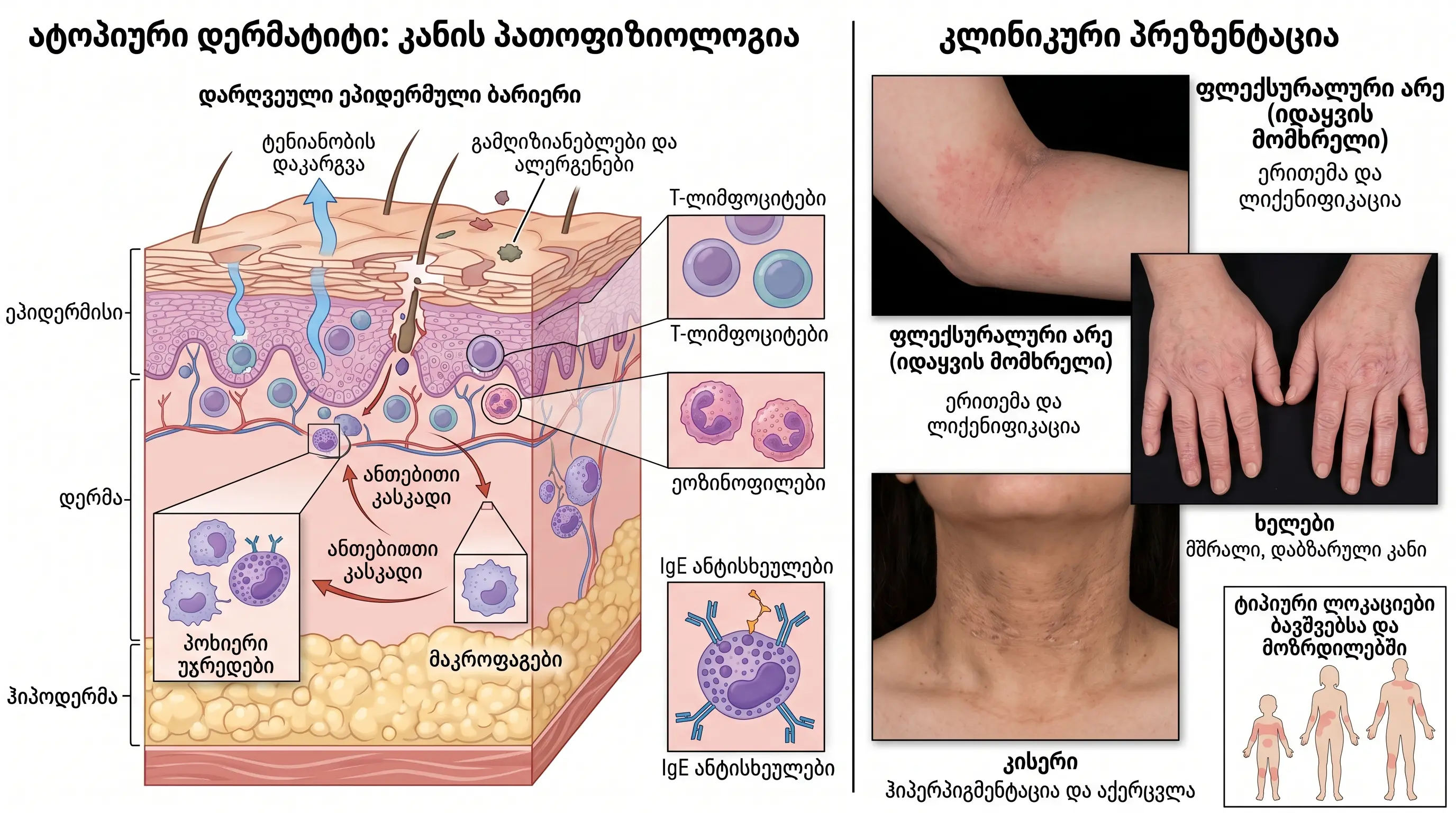
Epidemiological data:
- Children: Prevalence is 15-20%.
- Adults: Prevalence is 2-10%.
- Atopic dermatitis is a component of the atopic triad, which includes allergic rhinitis and bronchial asthma.
( Nutten, 2015, Annals of Nutrition and Metabolism )
4 factors of pathogenesis:
- Skin barrier dysfunction - filaggrin deficiency → disruption of the epidermal barrier;
- Immune dysregulation - enhancement of Th2-directed immune response;
- Microbiome imbalance - colonization of Staphylococcus aureus;
- Neurogenic inflammation - a cycle of itch intensification.
Age-related characteristics - localization:
| Age | Localization |
| Infants (0-2 years) | Face, scalp, axillary surfaces of limbs |
| Children (2-12 years old) | Curved surfaces of the elbow and knee |
| Adults (12+ years) | Hands, feet, neck, eyelids |
5-step treatment approach:
1 Basic therapy (for all patients):
- Emollients (moisturizing creams) 2-3 times a day;
- Identifying and avoiding triggers;
- Using a mild, unscented soap.
2 Topical anti-inflammatory therapy:
- Corticosteroids (depending on severity);
- Calcineurin inhibitors (tacrolimus, pimecrolimus);
3 Phototherapy:
- Narrow-band UVB;
- PUVA therapy.
4 Systemic therapy (severe cases):
- Cyclosporine;
- Methotrexate;
- Azathioprine.
5 Biological therapy (refractory cases):
- Dupilumab (anti-IL-4/IL-13 monoclonal antibody);
- Tralokinumab (anti-IL-13);
- New JAK inhibitors (abrocitinib, upadacitinib).
Sun allergy
This is an abnormal reaction of the skin to ultraviolet (UV) radiation. The term "sun allergy" encompasses several different clinical entities. 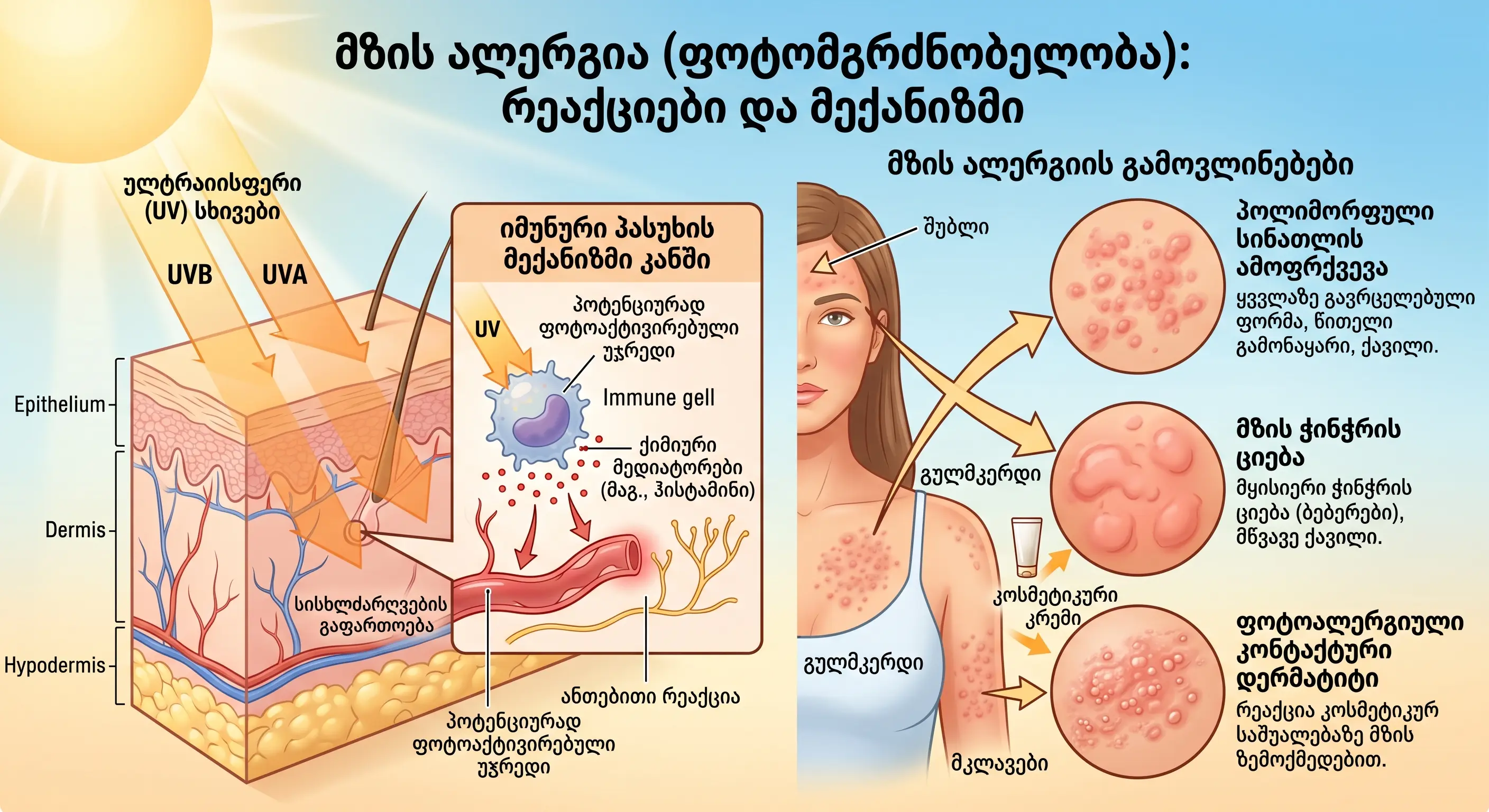
Its 3 main forms:
1. Polymorphic Light Eruption (PLE)
- The most common form, affecting 10-20% of the population.
- It is characterized by itchy papules, vesicles, and plaques.
- Localization : sun-exposed areas (décolleté, shoulders, hands).
- It appears in spring and early summer.
- Reason: The skin is not yet adapted to sunlight.
2. Solar urticaria
- A rare condition.
- Ultraviolet (UV) radiation causes instant hives.
- The rash disappears within minutes of exposure to the shade.
- It develops through an IgE-mediated mechanism.
3. Photoallergic contact dermatitis
- It develops as a result of the interaction of a substance applied to the skin and ultraviolet radiation, which creates an allergen.
- Common triggers are:
- Some sunscreen ingredients (e.g., oxybenzone);
- Antibiotics (e.g., tetracycline);
- Nonsteroidal anti-inflammatory drugs (eg, ketoprofen);
- It's perfume.
5 ways to prevent sun allergies:
- Sunscreen - broad spectrum, SPF 50+, UVA/UVB;
- Avoid peak hours - 11:00-16:00;
- Protective clothing - long sleeves, wide-brimmed hat;
- Gradual photoadaptation - gradual increase in sun exposure in spring;
- Preventive phototherapy - under the supervision of a doctor, before the start of the season.
Allergy medicine
Allergy pharmacotherapy includes different groups of drugs that act at different stages of the allergic cascade.

6 main groups of allergy medications:
- Mechanism of action : Competitive blockade of H1 histamine receptors.
- I generation (sedative):
- Representatives: diphenhydramine, chlorpheniramine.
- Disadvantage: Causes drowsiness and sedation.
- Generation II (non-sedating): Recommended as first-line drugs.
- Representatives: Alerfacit, Cetec, Loratadine, Fexofenadine, Desloratadine, Bilastine.
2 Intranasal corticosteroids
- Status: The most effective remedies for treating allergic rhinitis.
- Drugs: Naphtha, fluticasone, budesonide.
- Effect: Reduces inflammation, swelling, and secretion of the nasal mucosa.
3 Leukotriene receptor antagonists
- Drug: Montelukast.
- Use: in combined forms of allergic rhinitis and bronchial asthma.
- Advantage: One drug is used to treat both diseases.
4 Mast cell stabilizers
- Drug: cromoglycine (sodium cromoglycate).
- Action: Inhibits mast cell degranulation.
- Use: For prophylaxis, before contact with allergen.
5 Epinephrine autoinjector (EpiPen)
- Purpose: Used in the treatment of anaphylaxis - a life-threatening systemic reaction.
- Action: Instant.
- Application : performed on the outer surface of the thigh.
- Importance: Timely application is vital.
6 Topical medications (for skin allergies)
- Corticosteroid creams/ointments.
- Calcineurin inhibitors.
- Antihistamine gels.
- Moisturizing emollients.
Allergy treatment
Allergy treatment involves three main areas. The comprehensive treatment plan is individualized and depends on the type of allergy, its severity, and the patient's comorbid conditions. 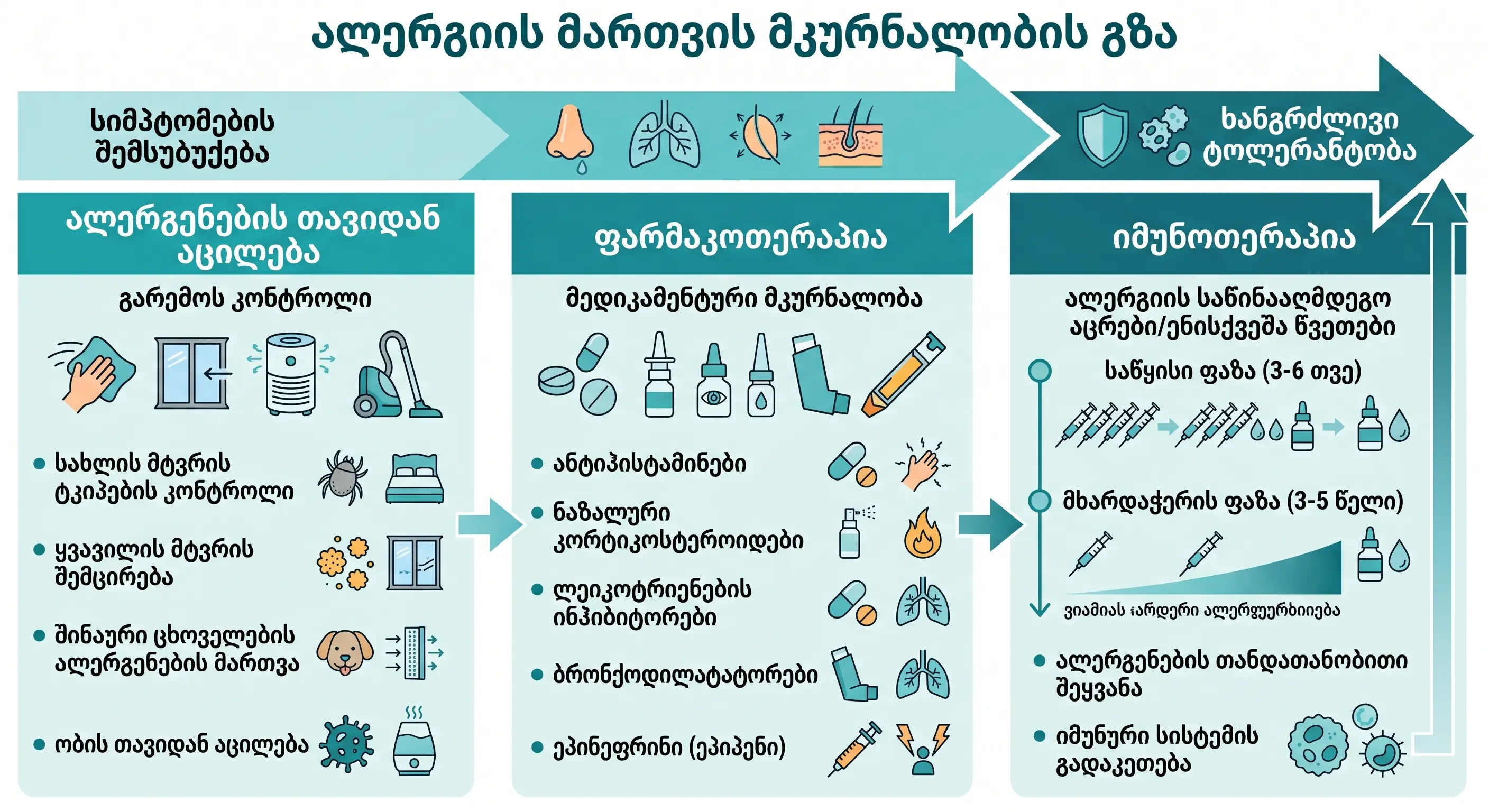
3 strategic directions of treatment:
Direction 1: Allergen elimination and environmental control
This is the first and most important step in treatment.
- In case of food allergy:
- Complete elimination of the allergen from the diet;
- Carefully study product labels;
- Cross-contamination prevention.
- In case of respiratory allergy:
- Use of HEPA filters (in air conditioners, air purifiers);
- Using hypoallergenic covers (on mattresses, pillows);
- Humidity control (maintain <50%);
- Regular wet cleaning and vacuuming (with a HEPA filter).
Direction 2: Pharmacotherapy
(For a detailed description, see the section "Allergy Medications")
Direction 3: Allergen-specific immunotherapy (AIT)
- Status: This is the only method that can change the course of allergic disease.
- Principle: Delivering gradually increasing doses of the allergen to the body.
- Duration: The course of treatment lasts 3-5 years.
- Two forms:
-
- SCIT - subcutaneous injections (performed in an allergist's office);
- SLIT - sublingual drops/tablets (taken at home).
- Proven effects:
- Significant reduction in symptoms;
- Reducing the need for medications;
- Prevention of new sensitizations;
- In children: prevention of progression of allergic rhinitis to bronchial asthma.
( Durham et al., 1999, NEJM; Jacobsen et al., 2007, Allergy )
Biological therapy - a new era:
| Drug | Target | Purpose |
| 1. Omalizumab | Anti-IgE | Severe asthma, chronic urticaria |
| 2. Dupilumab | Anti-IL-4/IL-13 | Atopic dermatitis, asthma, rhinosinusitis |
| 3. Mepolizumab | Anti-IL-5 | Eosinophilic asthma |
| 4. Benralizumab | Anti-IL-5R | Severe eosinophilic asthma |
Photos of the rash
Visual recognition of allergic rashes is an important part of making an accurate diagnosis. Below is a clinical description of the main types of allergic rashes.

5 main types of visual descriptions:
1. Urticaria (hives)
- Appearance: Raised, pink or red blisters (wheals).
- Size: from a few mm to a few cm.
- Surface: smooth, skin-colored.
- Itching: almost always.
- Peculiarity: migratory nature - disappears in one place, appears in another.
2. Atopic dermatitis
- Appearance: Erythematous, scaly plaques.
- Localization: curved surfaces (inner side of elbow, knee).
- Chronic phase: lichenification (thickening of the skin, increased pigmentation).
- Accompanying sign: excoriations due to intense itching.
3. Contact dermatitis
- Appearance: sharply demarcated erythema, vesicles or bullae.
- Localization: in the area of contact with the allergen.
- Examples:
- Eyeglass frame-shaped rash → nickel allergy;
- Hand eczema → latex allergy;
- Circular rash on the wrist → watch allergy.
4. Angioedema
- Appearance: Deep, asymmetrical swelling.
- Itching: Usually not (unlike urticaria).
- Localization: lips, eyelids, tongue, larynx.
- Danger: Airway obstruction → life-threatening.
5. Drug eruption
- Appearance: Morbidiform (measles-like) rash.
- Spread: Starts on the body → spreads to the extremities.
- Time: 7-14 days after taking the medication.
- Common triggers:
- Antibiotics (amoxicillin, sulfonamides);
- Nonsteroidal anti-inflammatory drugs;
- Antiepileptic drugs;
- Aspirin.
Note: Self-diagnosis of allergic rashes based on photos is for informational purposes only. For an accurate diagnosis, consultation with an allergist or dermatologist is necessary.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. You should consult a qualified healthcare professional before making any medical decisions.